
Sarepta Presents 48-Week Data At World Muscle Society Congress Long-term safety and efficacy results were presented this Saturday at the WMS Congress in Persh, Australia. We had already learned from a press release of top-line results October 3rd that results were positive: 50mg/kg treated patients remained stable- perhaps improved on the 6MWT- and treatment delayed patients appeared to have stabilized; dystrophin expression improved across all cohorts. While there are still questions remaining, the overall picture from Saturday’s presentation appears positive. It is unfortunate we were unable to attend or view the live discussions.
The primary endpoint is percent dystrophin positive fibers, with a clinical outcome measured by the 6-minute walk test (6MWT). The three original cohorts have become two active treatment arms of either 30mg/kg or 50mg/kg eteplirsen. It is important to note many later analyses exclude two patients from the 30mg/kg arm due to their initial rapid deterioration. As it turns out, the two are identical twins. The boys remain on study and continue to receive drug as well as monitoring. Pulmonary function of both subjects have remained stable through the 48-week extension.
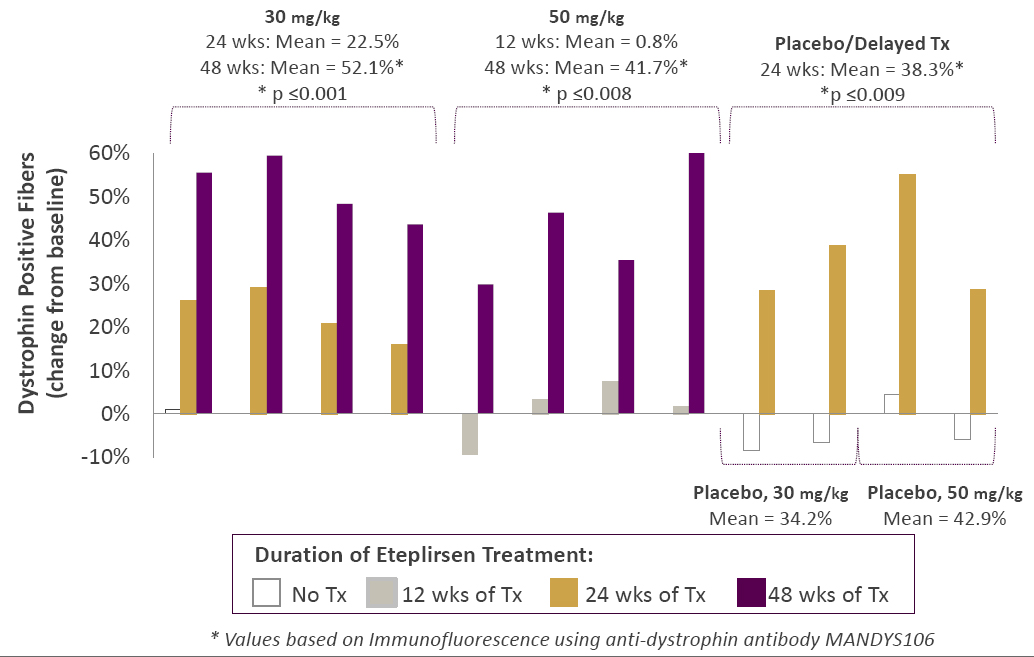
Below is a key piece of data describing individual dystrophin levels showed robust data. Increase in dystrophin positive fibers occurred in all 12 patients in a clear, time-dependent manner. No dose-response is apparent.
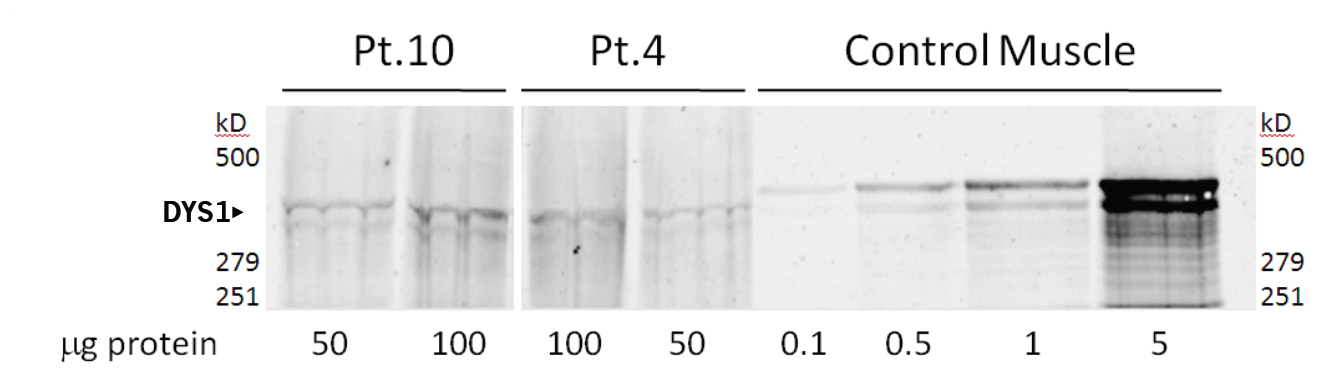
Additional measures including immunofluorescence, western blot, and RT-PCR all confirmed production of new dystrophin. A bit of fuss was made over the apparently low level of protein seen in the western blot and low RNA in the PCR assay. 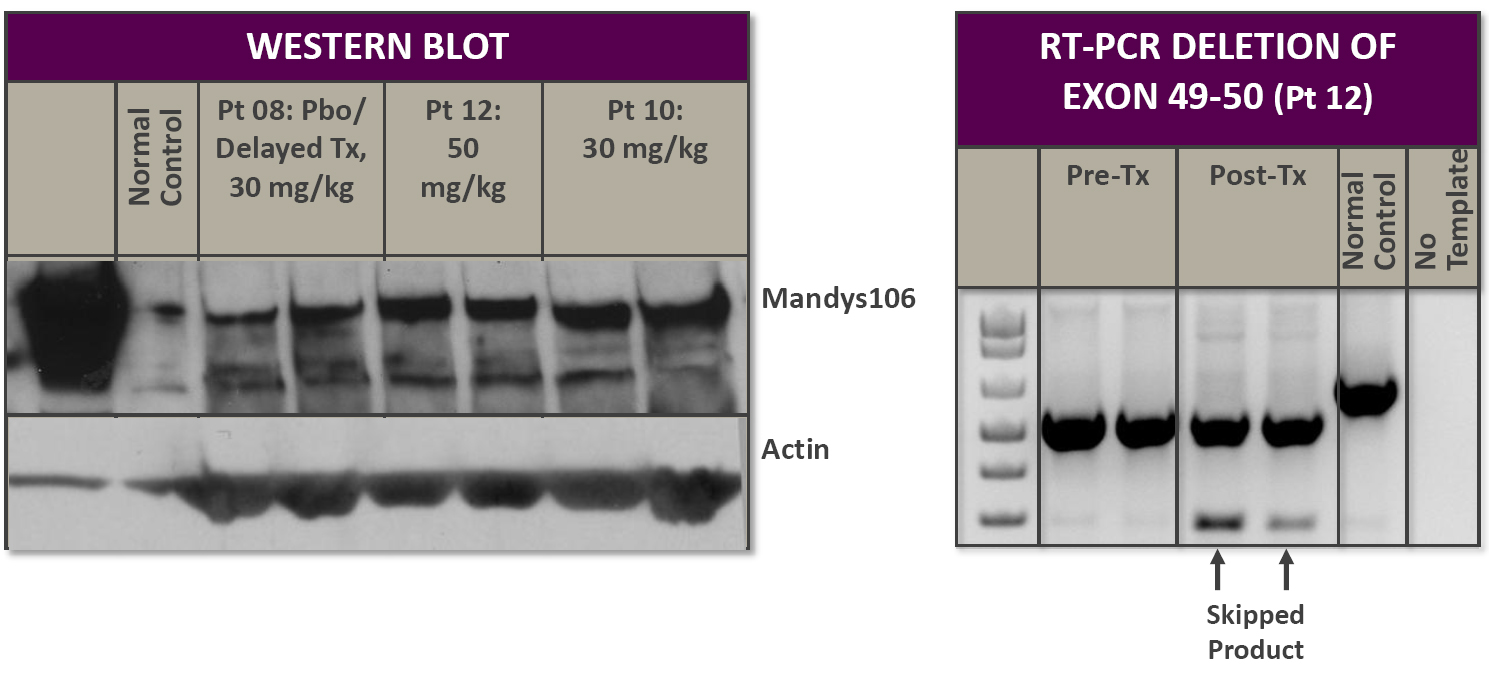
If we take a look at PRO051 from Prosensa, we can see that similarly low amounts of dystrophin are detected. This blot is from patient samples taken at 24 weeks. Notice the high amounts of protein loaded in each lane for patients compared to control.
What’s lacking are individual 6MWT scores, but this is because data is still being collected in the trial and the company is attempting to limit bias from parents influencing their children’s performance . The apparent improvement from 36-week to 48-week for both the 50mg/kg and treatment-delayed arms may simply be a blip and require further assessment. We have the mean data, now it is important to know if some boys fare much better, or worse, than others. The company will need to be more forthcoming with this. In particular, why is the 30mg/kg arm completely absent? Why isn’t the delayed treatment arm broken into 30mg/kg vs. 50mg/kg? It would be fantastic to see curves for each of the 12 patients. Unfortunately, we will likely have to wait to see these results.
In the end, eteplirsen maintains its crucial safety profile. There are no signs of kidney, liver, muscle, cardiac, or other measured toxicities. But as with any treatment where new proteins are introduced into the body, eteplirsen can potentially elicit an immune reaction. For this reason, all study participants had been tested for immunogenicity against dystrophin. Steroids taken by most DMD patients also appear to lessen the risk of a reaction.
The big question now is whether Sarepta will be able to secure an Accelerated Approval path for eteplirsen. The need is compelling and the results look good, but was the trial “adequate and well controlled”? This is the subject of heated debate. On the one hand, there is no arguing eteplirsen is active; it induced dystrophin formation in 100% of treated patients. And amazingly, the course of disease appears to have changed for the four delayed treatment patients. Yet of 8 patients who received drug for the entire 48-weeks, only 4 stabilized (that’s assuming all 4 boys in the 50mg/kg arm did well). And within this small group, evidence from a slew of family videos show boys previously limited by their disease to be thriving.
Up-coming Developments:
Later this week we hope to learn substantially more in a couple investor calls hosted by Wedbush with DMD expert Dr. David McDonald on Wednesday October 17, and CEO, Chris Garabedian, and Ed Kaye, CMO on Thursday October 18.
While investors agonize over the trial results, manufacturing of eteplirsen is becoming increasingly important. A contract manufacturer has been brought in to assist with scaling up production to commercial levels. Any details of Sarepta’s manufacturing capabilities would be welcome.
Perhaps the most important upcoming event will be Sarepta’s post Phase II meeting with the FDA either late this year or early 2013. Management will press their case for a quick path to market; with in months, we will know if the FDA is in agreement. Accelerated approval would be unprecedented for a trial of this size. The Agency will be under enormous pressure from advocacy groups as well as politicians to make the drug available. At the same time, it is tasked with ensuring the public’s safety. As of right now, with such a small number of test subjects, AA is certainly not a slam-dunk proposition. The end of Phase II meeting will provide clarity on this crucial matter.
An additional set of 6MWT data may also become available in December- this one at 60 weeks. With few patients, every data point bares increased importance. The 60-week time-point has the potential to confirm what appears to be a reversal in declining 6MWT scores of the delayed treatment cohort. In our view, this would demonstrate an amazing clinical benefit. The test can also confirm early signs of improvement in the 50mg/kg group; taken together, they have the potential to offer strong support for accelerated approval.
There is a lot to look forward to in the ensuing months. We remain bullish on Sarepta and believe it is undervalued relative to peers.
Disclosure: Author is Long SRPT













Do you happen to know what time the Wedbush meeting would be at on wednesday?
I don’t have those details- sorry
I get the sense with this data that the drug takes 12-24 weeks to make a meaningful impact, but that 24+ weeks it appears to have a clinically significant improvement. I wonder what 60, 80, 100 weeks would tell us?
Yep- I think those will be important numbers. will be fantastic if see continued improvement
Jason,
Solid report. Will this trade sideways until the overhang of AA and manufacturing are removed.
Thanks.
Greg
I really have no idea how it’ll trade. I think the Wedbush meetings in the next couple days may give the stock a push. But yeah, those two will be crucial.
One thing I forgot to mention is GSK/Prosensa is wrapping up a Phase II dose assessment study this month. Many investors may be waiting to see these results before deciding. http://clinicaltrials.gov/ct2/show/NCT01462292
Wedbush call with DMD expert today at 4 PM EST
Thanks
Any noteworthy updates from the wedbush call? Thanks.
During the Wedbush call SRPT said that “Cogs are closer to the biological model.” What does that mean? Are they saying that the COGS will be higher, lower or in line with those of other drug manufacturers.
so COGS will be closer to AMGN than CELG, more like mid double digits than mid single digits
Does anyone have an idea of how long it should take for SRPT to be in a position to manufacture the drug so as to meet FDA requirements and the needs of DMD pts? I assume SRPT can’t file for approval until the manufacturing issues are resolved.
based on mgmt comments at the recent parentproject Q&A, SRPT is in the process of working on mid-scale manufacturing- enough to supply a pivotal trial. They will not ramp to large scale until after meeting w/ the FDA Jan/Feb. If things go well, there could be a parallel ramp-up of both mid and large scale.
Neither scale-ups will be complete until 2014.
I do not know what the FDA will require of SRPT before allowing a regulatory filing in terms of manufacturing.